Ovarian cysts are fluid-filled sacs that develop in, or on the surface of your ovaries. They’re quite common and occur both before and after the menopause. They often don’t cause symptoms and are usually benign (non- cancerous). However, if the ovary twists because of the cyst (known as torsion), or the cyst leaks or bleeds into itself, they may cause pain in your abdomen (tummy) or pelvis.
Types of ovarian cyst
There are lots of different types of ovarian cysts. These can be broadly split into two groups to help explain how they develop: functional cysts and pathological cysts.
Functional cysts
Most ovarian cysts are functional cysts. This means that they develop as part of your usual menstrual cycle.
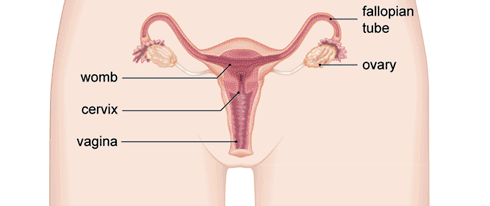
Each month your ovary produces several follicles (lumps filled with fluid), one of which will mature and release an egg. After the egg is released, the follicle normally transforms into something called the corpus luteum. The corpus luteum releases specific hormones that help the lining of your uterus develop and mature so it is ready to receive a fertilised egg. If the egg isn’t fertilised, the corpus luteum begins to break down. This happens after around 14 days.
Different types of functional cysts can grow at different stages in your cycle.
If a follicle doesn’t release an egg, it can carry on growing and develop into a cyst. This is called a follicular cyst. If the corpus luteum doesn’t break down after the egg is released, it can close back up and continue to grow. This is called a corpus luteal cyst.
Pathological cysts
These don’t develop as a result of anything to do with the usual function of your ovary. They may happen because of an overgrowth of cells or because of a particular condition, such as endometriosis. There are different types depending on the type of cell they start in.
Pathological cysts are also sometimes called tumours, but this does not necessarily mean that they are cancerous. Rarely an ovarian cyst can be cancerous (malignant).
Symptoms of ovarian cysts
Most ovarian cysts don’t cause any symptoms, so you may not even realise you have one. However, depending on the type you have, it’s possible you may:
- have pain or discomfort in your lower abdomen (tummy) or pelvis (between your hip bones)
- feel pain during sex
- need to pass urine more often or urgently
- find it more difficult to pass bowel movements or feel pressure in your back passage that makes you feel you need to go to the toilet
- feel bloated
- get indigestion or heartburn, or feel very full after you eat
- have painful periods, or a change in the pattern of your periods
These can be symptoms of other problems as well as ovarian cysts. If you have any of these symptoms or are worried, see your consultant for advice.
Ovarian cysts and pelvic inflammatory disease can have similar symptoms, but the two conditions are very different. Ovarian cysts aren’t caused by an infection, but pelvic inflammatory disease is – mostly sexually transmitted infections (STIs). Pelvic inflammatory disease can cause different symptoms, including:
- an abnormal vaginal discharge that may be smelly
- irregular periods, bleeding between periods or having heavier periods than usual
- pain when you pass urine
- a high temperature (over 38ºC)
- feeling sick or vomiting
If you have any of these symptoms, ask your consultant for advice.
Diagnosis of ovarian cysts
Most ovarian cysts don’t cause any symptoms so you may only find out you’ve got one if you’re having other tests such as an ultrasound scan.
If you see your consultant because you’ve got symptoms of an ovarian cyst, they’ll examine your abdomen (tummy). Your consultant may also examine you internally in a vaginal examination. If your consultant thinks you have a cyst that needs investigating further, you may need to have the following tests.
- Transvaginal ultrasound – an ultrasound probe placed into your vagina produces a clear picture of your ovaries.
- Transabdominal ultrasound – a scan over your lower abdomen to check for any problems around your pelvic area.
- Blood tests. You might have a blood test to help rule out cancer.
Transvaginal ultrasound is the most reliable test for an ovarian cyst. You may have an abdominal ultrasound as well if the cyst is large or to rule out other conditions.
If you’ve been through the menopause, your doctor may do a blood test for a substance called CA-125. If the level of CA-125 in your blood is raised, it could mean you have ovarian cancer. However this isn’t always the case. Your CA-125 levels may be raised if you have other benign (non-cancerous) conditions. Some of these conditions are common before you have your menopause, such as endometriosis and fibroids, so the test is less useful if you haven’t been through the menopause yet. However, if you are pre-menopausal but your doctor cannot be completely sure from an ultrasound that you have a simple, fluid-filled cyst, they may do this test.
If you’re under 40, your doctor may do other blood tests called LDH, AFP and HCG. These can show if a cyst is a type of cancer called a germ cell tumour. These are rare and you’re very unlikely to have one – the blood tests are just a precaution.
Treatment of ovarian cysts
If you have an ovarian cyst, your treatment options will depend on a number of things. As well as your personal preference, these include:
- the type of cyst
- how large it is
- whether you have symptoms
- whether you’ve had your menopause
Pre-menopausal women
In women who are still having periods, cysts less than 5cm across usually go away on their own within two to three menstrual cycles. If you don’t have any symptoms and your ovarian cyst is this small, you won’t need any treatment and you probably won’t need any further tests. If you start having symptoms, go back to your consultant.
If your ovarian cyst is larger (between 5 and 7cm), your consultant may suggest you have a repeat ultrasound scan up to a year later, to make sure it hasn’t grown. Ultrasound scans are the best way of looking at simple ovarian cysts that are just filled with fluid. If the ultrasound is not clear, or part or all of the cyst appears to be solid tissue, your doctor may suggest you have a magnetic resonance imaging (MRI) scan. A MRI scan uses magnets and radio waves to produce images of the inside of your body. If you start having symptoms in the meantime, go back to your consultant.
Post-menopausal women
In women who have had their menopause, about half of those cysts less than 5cm across go away on their own within three months. So if your cyst isn’t causing problems, your consultant is most likely to ask you to have a repeat ultrasound scan four to six months later to check it hasn’t grown. If it hasn’t, you may have another ultrasound four to six months after that to monitor it. You’ll also have a repeat CA-125 blood test (see the Diagnosis section for more information). If there’s still no change, your consultant may suggest that you have no further follow-up.
Pregnancy
Cysts during pregnancy nearly always go away on their own. At around 16 to 20 weeks, more than nine out of ten cysts will have disappeared. Your doctor will only consider removing it if it is causing you pain or growing very quickly.
Surgery
If your cyst is larger or causing symptoms, your doctor is likely to suggest you have surgery to remove it. Larger means more than 5cm across if you are past your menopause, or more than 7cm across if you are still having periods. Your doctor is also more likely to suggest surgery if your cysts are complex. This is when parts of the cyst are solid rather than liquid.
Even if your cyst is less than 7cm across, your doctor may suggest surgery if you are pre-menopausal and your cyst doesn’t go away on its own after several menstrual cycles.
There are two ways of carrying out surgery for an ovarian cyst:
- keyhole surgery (laparoscopy)
- open surgery (laparotomy)
You’re most likely to be offered keyhole surgery. This type of operation is carried out through very small incisions (cuts) and the surgeon uses a tube with an eyepiece (telescope) and a camera to see inside the body. The recovery time is usually quicker than for open surgery with a lower risk of complications and pain after the operation.
Your consultant may prefer to do open surgery if you have a very large complex cyst. You’ll also have open surgery if there is any concern that the cyst may be cancerous. Open surgery needs a larger incision so it usually takes a bit longer to recover from the operation.
Causes of ovarian cysts
Doctors don’t yet know exactly why some women develop ovarian cysts. However, there are some things that seem to increase your chance of getting them.
If you take progestogen contraception, it may increase your risk of getting functional cysts. Examples of progestogen contraception include the progestogen-only pill, the intrauterine system (Mirena) or the contraceptive implant (nexplanon).
Some hormones that are used to treat infertility can trigger functional cysts to develop in your ovaries. If you’re taking the medicine tamoxifen for breast cancer, you may develop cysts, but they usually go away when you finish treatment.
If you’re pregnant, ovarian cysts can form as your hormone levels change during your pregnancy.
Having an underactive thyroid can increase your risk of getting ovarian cysts. You may be at risk of ovarian cysts if you have endometriosis.
If you smoke, it may increase your risk of getting functional ovarian cysts.
Complications of ovarian cysts
Rarely, a cyst can cause your ovary to twist, which is called torsion. Or the cyst itself can suddenly burst (rupture). Both of these problems can cause severe pain in your abdomen (tummy). You may also have a fever and feel sick or vomit.
These complications aren’t common. But if you have been diagnosed with a cyst and develop these symptoms, go to Accident and Emergency straightaway. You may need to have surgery.
Do ovarian cysts affect fertility?
Ovarian cysts don’t usually affect your fertility. But if you need to have surgery to remove a cyst, this could affect your ability to have a child.
Most ovarian cysts are functional ones. These are usually small and will go away without treatment. In some cases though, ovarian cysts need treating with surgery.
If you need to have surgery, if at all possible, only the cyst will be removed and your ovary won’t be. However, if your cyst is very large or if your ovary has twisted (torsion), it may need to be removed.
If you need to have your ovary removed, you’ll still be able to have a child if you have one ovary left, or even part of an ovary. If, while operating, your surgeon finds that the cyst is cancerous, you may need to have your ovary removed. If you are found to have ovarian cancer, it’s possible that you may need to have your womb removed (hysterectomy) as well. But your surgeon will do this in a separate operation unless you have agreed to it first. If you’ve had a hysterectomy, you won’t be able to get pregnant.
Remember that ovarian cancer is very unlikely in a pre-menopausal woman with an ovarian cyst.
You’ll have the chance to discuss all the options available to you with your consultant before you have surgery, so make sure you talk to them about your fertility and how important it is to you. Your surgeon won’t be able to give you a definite guarantee beforehand in case there are unexpected complications. But during the operation they’ll make every effort to ensure your ovary doesn’t need to be removed.
Does having an ovarian cyst mean I have cancer?
Most ovarian cysts aren’t cancerous. In medical language, they aren’t malignant – they are benign.
About one in 1,000 ovarian cysts are found to be cancerous in women who have not yet gone through the menopause.
About three in 1,000 ovarian cysts turn out to be cancerous in women over the age of 50.
However, your risk of ovarian cancer with an ovarian cyst also depends on a number of factors, including:
- the exact type of cyst you have
- if you’ve had, or are able to have children
- if you have had breast or ovarian cancer (or relatives who have)
You’ll have a number of tests to check whether your ovarian cyst is benign or cancerous. See our section on diagnosis for more information.
What’s the difference between PCOS and ovarian cysts?
At some point in their reproductive years, as many as one in three women have cysts on their ovaries that can be seen on ultrasound scan. But this is not the same thing as polycystic ovary syndrome (PCOS). Women with cysts on their ovaries often have no symptoms and the cyst frequently goes away on its own.
Women with polycystic ovary syndrome (PCOS) may have lots of cysts on their ovaries, but they also have abnormalities in the way their bodies produce and manage sex hormones. PCOS is a collection of symptoms that includes cysts on the ovaries. As well as cysts, women with PCOS may:
- produce higher than normal levels of male hormones (androgens)
- be less sensitive to insulin than normal
- have higher than normal levels of a pituitary hormone called luteinising hormone
- have higher than normal oestrogen levels
So there are a number of different possible hormone imbalances linked to PCOS. These differences in hormone levels cause a number of different symptoms. These include:
- infertility
- increase in facial and body hair (hirsutism)
- lack of periods (amenorrhoea) or infrequent periods
- acne
- baldness
- weight gain
On average, women with PCOS have ovaries three times normal size but confusingly, some women with POS don’t have cysts on their ovaries at all. Not ovulating and having the hormone imbalances listed above is enough for a diagnosis.
If your consultant is investigating you for this condition, you’ll have a number of blood tests. These will have to show some of the hormone imbalances listed above in order to get a definite diagnosis of PCOS.